|
Page 33.
For the sadness in legitimate humour
consists in the fact that honestly and without deceit it
reflects in a purely human way upon what it is to be a
child.
- Soren Kierkegaard
Very early in life every child
concludes, 'I'm not OK.' He makes a conclusion about his
parents, also: 'You're OK'. This is the first thing he
figures out in his life-long attempt to make sense of
himself and the world in which he lives. This position,
I'm not ok - you're ok, is the most deterministic
decision of his life. It is permanently recorded and
will influence everything he does. Because it is a
decision it can be changed by a new decision. But not
until it is understood.

In order to support these contentions I
wish to devote the first part of this chapter to an
examination of the situations of the newborn, the young
infant, and the growing child, in both the preverbal and
verbal years. Many people insist they had a 'happy
childhood' and concluded nothing like I'm not ok -you're
ok. I believe strongly that every child concludes it.
'happy childhood' notwithstanding. First, I wish to
examine the situation of his entry into life and to
point to the evidence that the events of his birth and
his infant life are recorded, even though they are not
remembered.
In this connexion we note again
Penfield's conclusions that the brain performs three
functions: (1) recording, (2) recalling, and (3)
reliving. Although recall from the earliest period of
life is not possible, we have evidence that we can and
do relive the earliest experiences in the form of
returning to the feeling state of the newborn infant.
Because the infant cannot use words, his reactions are
limited to sensations, feelings, and perhaps vague,
archaic fantasies. His feelings are expressed by crying
or by various body movements that indicate either
distress or comfort. His sensations and fantasies,
though ineffable because of his wordlessness at the time
they were recorded, do replay occasionally in dreams in
later life.
To illustrate: A patient reported a
dream that had recurred throughout her life. Each time
she had this dream, she awoke in a state of extreme
panic, with rapid heartbeat and heavy breathing. She
struggled to describe the dream but she could not find
words for it. In one attempt at description she said she
thought she felt as if she were 'just a tiny, little,
small speck, and big, huge, round, cosmic things were
swirling around me, like great spirals, getting bigger
and bigger, and threatening to engulf me, and I just
seemed to disappear in this vast, enormous thing'.
Though her report was accompanied by her observation
about losing her identity, the nature of the extreme
panic would seem to indicate there may have been a fear
of losing her life, as a primary biological reaction to
the threat of death.
Some time later she again reported the
dream. It was the first time she had dreamed it for
about a year. She had been traveling, and she and her
husband had eaten lunch in an out of-the-way restaurant
with an atmosphere of a higher quality than the food's.
She did not feel well when they returned to their hotel,
so she lay down for a nap. She fell asleep. It was not
long before she awoke in the panic of this same dream.
She also had severe stomach cramps, which 'had me all
doubled up in pain'. No recent event had been
particularly anxiety-provoking, and the panic dream
seemed to have some direct connexion with the extreme,
primordial gut pain. The dream was still indescribable;
however, she did report another sensation, the feeling
that she was suffocating.
Page 34.
Certain information about the patient's
mother helped to suggest a possible origin of this
dream. The mother, a large, plump woman, had breast-fed
her children and had held to the idea there was no
problem that eating would not cure. Her idea of
well-cared-for children was well-fed children. She also
was an aggressive, domineering woman. We deduced (which
is all we can do) that the dream had its origin in a
time before the patient had words, since she could not
describe the content. The association with the belly
cramp suggested some connexion with an early eating
experience. The probability is that if, as an infant,
the patient had had enough, or had had a full feeling
and quit nursing, the mother would insist she have more.
(This was before the era of demand-feeding: 'fill up
now, it will have to last you'.) Feelings of
'dream-state' sleepiness, suffocation, and stomach
cramps could have been present. The content (the small
thing being engulfed by huge, cosmic things) could have
been a replay of the infant's perception of her
situation - herself, the small speck, being engulfed by
the huge, round things, mother's breasts, or the huge
presence of the mother herself.
This type of dream material lends
support to the assumption that our earliest experiences,
though ineffable, are recorded and do replay in the
present. Another indication that experiences are
recorded from the time of birth is the retention of past
gains. The infant's responses to external stimuli,
although at first instinctual, soon reflect conditioned
or learned (or recorded) experience. For instance, he
learns to look in the direction of mother's footsteps.
If all experiences and feelings are recorded, we can
understand the extreme panic, or rage, or fear we feel
in certain situations today as a reliving of the
original state of panic or rage or fear that we felt as
infants. We can think of this as a replay of the
original tape.
To understand the implications, it is
important to examine the situation of the infant. In
reference to Figure 7, we see a line representing a span
from the moment of conception to the age of five. The
first block of time is the nine months between
conception and biological birth. During these nine
months there occurred a beginning of life in the most
perfect environment the human individual may ever
experience. This way of life is referred to as a state
of symbiotic intimacy.
Page 35.
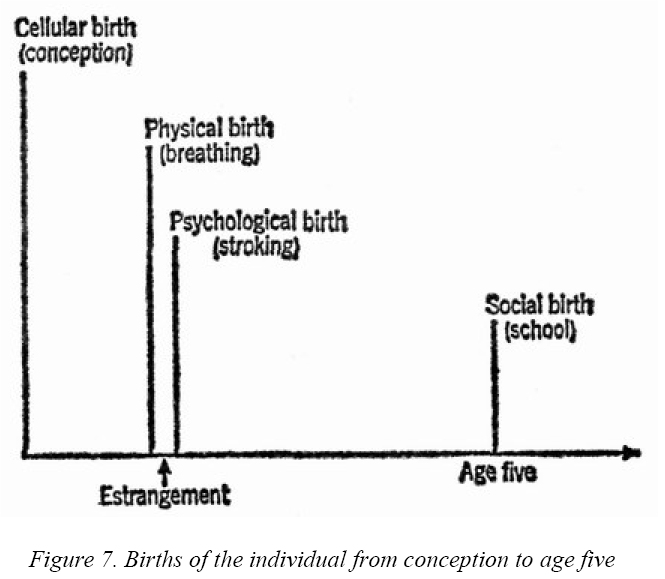
Figure 7. Births of the individual from
conception to age five
Then, at biological birth, the little
individual, within the brief span of a few hours, is
pushed out into a state of catastrophic contrast in
which he is exposed to foreign and doubtless terrifying
extremes of cold, roughness, pressure, noise,
nonsupport, brightness, separateness, and abandonment.
The infant is, for a short time, cut off, apart,
separate, unrelated. Common to the many theories about
the birth trauma is the assumption that the feelings
produced by this event were recorded and reside in some
form in the brain. This assumption is supported by the
great number of repetitious dreams of the 'drainage
pipe' variety which so many individuals experience
following situations of extreme stress. The patient
describes a dream in which he is swept from a body of
water of relative calm into a sewer or drainage pipe. He
experiences the feeling of increasing velocity and
compression. This feeling also is experienced in the
state of claustrophobia. The infant is flooded with
overwhelming, unpleasant stimulations, and the feelings
resulting in the child are, according to Freud, the
model for all later anxiety. {1}
Within moments the infant is introduced
to a rescuer, another human being who picks him up,
wraps him in warm coverings, supports him, and begins
the comforting act of 'stroking'. This is the point
(Figure 7) of Psychological Birth. This is the first
incoming data that life 'out there' isn't all bad. It is
a reconciliation, a reinstatement of closeness. It turns
on his will to live. Stroking, or repetitious bodily
contact, is essential to his survival. Without it he
will die, if not physically, then psychologically.
Physical death from a condition known as marasmus once
was a frequent occurrence in foundling homes where there
was a deprivation of this early stroking. There was no
physical cause to explain these deaths except the
absence of essential stimulation.
Page 36.
This painful on-again-off-again keeps
the infant in a constant state of disequilibrium. During
the first two years of life he does not have conceptual
'thinking' tools - words - to construct an explanation
of his uncertain status in his world. He is, however,
continually recording the feelings which grow from the
relationship between himself and others, primarily
mother, and these feelings are directly related to
stroking and non-stroking. Whoever provides stroking is
ok. His estimate of himself is unsure because his ok
feelings are transitory and continually being replaced
by not ok feelings. Finally the uncertainty convinces
him I'm not ok. At what point does the child make final
his decision as to the position, I'm Not Ok-You're Ok?
Piaget, {2} on the basis of meticulous
observations of infants and small children, believes
that the development of causality (what follows what)
begins in the early months of life and is acquired by
the end of the second year. In other words, data, in the
form of a jumble of impressions, begins accumulating in
certain sequential patterns, to a point where a
preverbal position, or conclusion, is possible. Piaget
says: 'In the course of the first two years of childhood
the evolution of sensorimotor intelligence, and also the
correlative elaboration of the universe, seem to lead to
a state of equilibrium bordering on rational thought.' I
believe this state of equilibrium, evident at the end of
the second year or during the third year, is the product
of the child's conclusion about himself and others: his
life position. Once his position is decided he has
something solid to work with, some basis for
predictability. Piaget says that these early mental
processes are not capable of 'knowing or stating truths'
but are limited to desiring success or practical
adaptation: If I'm not ok and you're ok, what can I do
to make you, an ok person, be good to me, a not ok
person? The position may seem unfavourable, but it is a
true impression, to the child, and it is better than
nothing. Thus the state of equilibrium. The Adult in the
little person has achieved its first mastery in 'making
sense of life', in solving what Adler called 'life's
central problem' - the attitude towards others -and what
Sullivan called the 'self-attitudes which are carried
forever by the individual'.
One of the clearest statements on the
development of positions is made by Kubie:
It is possible to make one certain
deduction: namely, that early in life, sometimes within
the earliest months and sometimes later, a
central emotional position is frequently established ...
The clinical fact which is already evident is that once
a central emotional position is established early in
life, it becomes the affective position to
which that individual will tend to return automatically
for the rest of his days.
This in turn may constitute either the major safeguard
or the major vulnerability of his life. In fact the
establishing of a central emotional position may turn
out to be one of the earliest among the universals in
the evolution of the human neurotic process, since it
may start even in the pre-verbal and largely
pre-symbolic days of infancy ... Whenever the central
emotional position is painful ... the individual may
spend his whole life defending himself against it, again
using conscious, preconscious, and unconscious devices
whose aim it is to avoid this pain-filled central
position. {3} [Italics mine]
Page 37.
Kubie then raises the question as to
whether or not these positions are alterable later in
life. I believe they are. Although the early experiences
which culminated in the position cannot be erased, I
believe the early positions can be changed. What was
once decided can be undecided.
Transactional Analysis constructs the
following classification of the four possible life
positions held with respect to oneself and others:
1. I'm Not Ok-You're Ok
2. I'm Not Ok-You're Not Ok
3. I'm Ok-You're Not Ok
4. I'm Ok - You're Ok
Before I elaborate each position I wish
to state a few general observations about positions. I
believe that by the end of the second year of life, or
sometime during the third year, the child has decided on
one of the first three positions. The I'm not ok -
you're ok is the first tentative decision based on the
experiences of the first year of life. By the end of the
second year it is either confirmed and settled or it
gives way to Position 2 or 3: I'm not ok-you're not ok
or I'm ok-you're not ok. Once finalized, the child stays
in his chosen position and it governs everything he
does. It stays with him the rest of his life, unless he
later consciously changes it to the fourth position.
People do not shift back and forth. The decision as to
the first three positions is based totally on stroking
and non-stroking. The first three are nonverbal
decisions. They are conclusions, not explanations. Yet
they are more than conditioned responses. They are what
Piaget calls intellectual elaborations in the
construction of causality. In other words, they are a
product of Adult data processing in the very little
person.
I'm Not
OK-You're OK
This is the universal position of early
childhood, being the infant's logical conclusion from
the situation of birth and infancy. There is OK-ness in
this position, because stroking is present. Every child
is stroked in the first year of life simply by the fact
that he has to be picked up to be cared for. Without at
least minimal handling the infant would not survive.
There is also NOT-OK-ness. That is the conclusion about
himself. I believe the evidence points to the
overwhelming accumulation of not ok feelings in the
child, making logical (on the basis of the evidence he-
has) his not ok conclusion about himself. In explaining
Transactional Analysis to patients and nonpatients I
have found a generally that's it! response to the
explanation of the origin and existence of the not ok
Child. I believe that acknowledging the not ok Child in
each of us is the only sympathetic, thus curative, way
games can be analysed. Considering the universality of
games, the universality of the I'm not ok is a
reasonable deduction. Adler's break with Freud was over
this point: sex was not at the basis of man's struggle
in life, but rather feelings of inferiority, or not ok,
which were apparent universally. He claimed that the
child, by virtue of his small size and helplessness,
inevitably considered himself inferior to the adult
figures in his environment. Harry Stack Sullivan was
greatly influenced by Adler, and I was greatly
influenced by Sullivan, with whom I studied for the five
years preceding his death. Sullivan, whose central
contribution to psychoanalytic thought was the concept
of 'interpersonal relationships', or transactions,
claimed that the child built his self-estimate totally
on the appraisal of others, what he called 'reflected
appraisals'. He said:
Page 38.
The child lacks the equipment and
experience necessary to form an accurate picture of
himself, so his only guide is the reactions of others to
him. There is very little cause for him to question
these appraisals, and in any case he is far too helpless
to challenge them or to rebel against them. He passively
accepts the judgments, which are communicated
empathetically at first, and by words, gestures, and
deeds in this period ... thus the self attitudes learned
early in life are carried forever by the individual,
with some allowance for the influence of extraordinary
environmental circumstances and modification through
later experiences. {4}
In the first position the person feels
at the mercy of others. He feels a great need for
stroking, or recognition, which is the psychological
version of the early physical stroking. In this
position there is hope because there is a source of
stroking -you're ok - even if the stroking is not
constant. The Adult has something to work on: what must
I do to gain their strokes, or their approval? There are
two ways in which people may attempt to live out this
position.
The first is to live out a life script
{*} that confirms the not ok. It is written
unconsciously by the Child. The script may call for a
life of withdrawal, since it is too painful to be around
ok people. Thus a person may seek stroking through
make-believe and engage in an elaborate wish-life of if
1 and when I. Another person's script may call for
behaviour which is provoking to the point where others
turn on him (negative stroking), thus proving once
again, I'm not ok. This is the case of the 'bad little
boy'. You say I'm bad so I'll be bad! He may kick and
spit and claw his way through life and thus achieve a
fraudulent integrity with at least one constant he can
count on: I'm not ok - you're ok. There is a kind of
miserable sense in this, in that the integrity of the
position is maintained, but it leads to despair. The
ultimate resolution of this position is giving up
(leading to institutionalization) or suicide.
A more common way to live out this
position is by a counter-script (also unconscious) with
borrowed lines from the Parent: you can be ok, if. Such
a person seeks friends and associates who have a big
Parent because he needs big strokes, and the bigger the
Parent, the better the strokes, (ok strokes can only
come from ok people, and the Parent is ok, as it was in
the beginning.) This person is eager, willing, and
compliant to the demands of others. 'Some of our best
people' are where they are because of these efforts to
gain approval. However, they are committed to a lifetime
of mountain climbing, and when they reach the top of one
mountain they are confronted by still another mountain.
The not ok writes the script; the you're ok (and I want
to be like you) writes the counter script. Neither works
in producing happiness or a sense of lasting worth,
however, because the position has not changed. 'No
matter what I do, I'm still not ok.'
Once the position is uncovered and
changed, the achievements and skills that have resulted
from the counter script can serve the person well when
he builds a new and conscious life plan with the Adult.
Page 39.
I'm
NOT OK- You're Not OK
If all children who survive infancy
initially conclude I'm not ok-you're ok, what happens to
produce the second position, I'm not ok and neither are
you? What happened to the you're ok? What happened to
the source of stroking?
By the end of the first year something
significant has happened to the child. He is walking. He
no longer has to be picked up. If his mother is cold and
nonstroking, if she only put up with him during the
first year because she had to, then his learning to walk
means that his 'babying' days are over. The stroking
ceases entirely. In addition punishments come harder and
more often as he is able to climb out of his crib, as he
gets into everything, and won't stay put. Even
self-inflicted hurts come more frequently as his
mobility sends him tripping over. obstacles and tumbling
down stairs.
Life, which in the first year had some
comforts, now has none. The stroking has disappeared. If
this state of abandonment and difficulty continues
without relief through the second year of life, the
child concludes I'm not ok - you're not ok. In this
position the Adult stops developing since one of its
primary functions - getting strokes - is thwarted in
that there is no source of stroking. A person in this
position gives up. There is no hope. He simply gets
through life and ultimately may end up in a mental
institution in a state of extreme withdrawal, with
regressive behaviour which reflects a vague, archaic
longing to get back to life as it was in the first year
during which he received the only stroking he ever knew
- as an infant who was held and fed.
It is hard to imagine anyone going
through life without any stroking. Even with a
nonstroking mother there most certainly appeared persons
who were capable of caring for a person in this position
and who, in fact, did stroke. However, once a position
is decided, all experience is selectively interpreted to
support it. If a person concludes you're not ok, it
applies to all other people, and he rejects their
stroking, genuine though it may be. He originally found
some measure of integrity or sense in his early
conclusion; therefore new experiences do not readily
break it down. This is the deterministic nature of
positions. Also, the individual in this position stops
using his Adult with regard to his relationships with
others. Therefore, even in treatment, it is difficult to
reach his Adult, particularly in view of the fact that
the therapist also occupies the category you're not ok.
There is one condition in which I'm not
ok-you're not ok may be the initial position, rather
than secondary to the first. This is the condition of
the autistic child. The autistic child remains
psychologically unborn. Infantile autism appears to be
the response of the immature organism to catastrophic
stress in an external world in which there is no
stroking which gets through to him. The autistic child
is one, who in the critical early weeks of life, did not
feel himself to be rescued. It is as if he found 'nobody
out there' after his catastrophic expulsion into life.
Page 40.
Schopler {5} concludes there is a
physiological factor which combines with insufficient
stroking to produce the autistic child. The factor is
thought to be a high stimulus barrier so that the
stroking which is given does not register. He may not be
totally deprived of stroking, but he may be deprived of
his sensation of it, or an 'accumulation' of his
sensations of it. The infant is then seen by the parents
as a nonresponsive child (he doesn't like to be held, he
just lies there, he's different), and then even the
stroking which has been given is withheld because 'he
doesn't like to be held'. It is possible that vigorous
stroking (more than is given ordinarily) may have
overcome the barrier. Once I observed an
eleven-year-old, nonverbal, autistic boy evidence the
seeming perception of the I' M NOT OK-YOU'RE not ok
position by an intense, repeated hitting with his fist,
first his counsellor, and then his own head. It was as
if he were acting out his view of life: You're not ok
and I'm not ok. Let's smash both of us.
I'm OK-You're-Not OK
A child who is brutalized long enough by
the parents he initially felt were ok will switch
positions to the third, or criminal, position: I'm ok -
you're not ok. There is OK-ness here, but where does it
come from? Where is the source of stroking if you're not
ok? This is a difficult question considering that the
position is decided in the second or third year of life.
If a two-year-old concludes I'm ok, does this mean his
ok is the product of 'self-stroking', and, if so, how
does a small child stroke himself?
I believe this self-stroking does in
fact occur during the time that a little person is
healing from major, painful injuries such as are
inflicted on a youngster who has come to be known as
'the battered child'. This is the child who has been
beaten so severely that bones and skin are broken.
Anyone who has had a broken bone or massive bruises
knows the pain. Common in battered children are
extremely painful injuries such as broken ribs, smashed
kidneys, and fractured skulls. How does the every-breath
agony of broken ribs or the excruciating headache from
blood in the spinal fluid feel to a toddler? Every hour
five infants in this country receive injuries of this
kind at the hands of their parents.
I believe that it is while this little
individual is healing, in a sense 'lying there licking
his wounds', that he experiences a sense of comfort
alone and by himself, if for no other reason than that
his improvement is in such contrast to the gross pain he
has just experienced. It is as if he senses, I'll be all
right if you leave me alone. I'm ok by myself. As the
brutal parents reappear, he may shrink in horror that it
will happen again. You hurt me! You are not ok. I'm ok -
you're not ok. The early history of many criminal
psychopaths, who occupy this position, reveal this kind
of gross physical abuse.
Such a little person has experienced
brutality, but he has also experienced survival. What
has happened can happen again. I did survive. I will
survive. He refuses to give up. As he grows older he
begins to strike back. He has seen toughness and knows
how to be tough. He also has permission (in his Parent)
to be tough and to be cruel. Hatred sustains him
although he may learn to conceal it with a mask of
measured politeness. Caryl Chessman said, 'There is
nothing that sustains you like hate; it is better to be
anything than afraid.'
Page 41.
For this child the I'm ok - you're not
ok position is a life-saving decision. The tragedy, for
himself and for society, is that he goes through life
refusing to look inward. He is unable to be objective
about his own complicity in what happens to him. It is
always 'their fault'. It's 'all them'. Incorrigible
criminals occupy this position. They are the persons
'without a conscience' who are convinced that they are
ok no matter what they do and that the total fault in
every situation lies in others. This condition, which at
one time was referred to as 'moral imbecility', is
actually a condition in which the person has shut out
any incoming data that anyone is ok. For this reason
treatment is difficult, since the therapist is not ok
along with everyone else. The ultimate expression of
this position is homicide, felt by the killer to be
justifiable (in the same way that he felt justified in
taking the position in the first place).
The person in the I'm ok - you're not ok
position suffers from stroking deprivation. A stroke is
only as good as the stroker. And there are no ok people.
Therefore there are no ok strokes. Such a person may
develop a retinue of 'yes men' who praise and stroke him
heavily. Yet he knows they are not authentic strokes
because he has had to set them up himself, in the same
way he had to produce his own stroking in the first
place. The more they praise him the more despicable they
become, until he finally rejects them all in favour of a
new group of yes men. 'Come close so I can let you have
it' is an old recording. That's the way it was in the
beginning.
I'm OK-You're Ok
There is a fourth position, wherein lies
our hope. It is the I'm ok - you're ok position. There
is a qualitative difference between the first three
positions and the fourth position. The first three are
unconscious, having been made early in life. I'm not ok
- you're ok came first and persists for most people
throughout life. For certain extremely unfortunate
children this position was changed to positions two and
three. By the third year of life one of these positions
is fixed in every person. The decision as to position is
perhaps one of the first functions of the infant's Adult
in the attempt to make sense out of life, so that a
measure of predictability may be applied to the
confusion of stimuli and feelings. These positions are
ar rived
at on the basis of data from the Parent and Child. They
are based on emotion or impressions without the benefit
of external, modifying data.
The fourth position, I'm ok-you're ok,
because it is a conscious and verbal decision, can
include not only an infinitely greater amount of
information about the individual and others, but also
the incorporation of not-yet-experienced possibilities
which exist in the abstractions of philosophy and
religion. The first three positions are based on
feelings. The fourth is based on thought, faith, and the
wager of action. The first three have to do with why.
The fourth has to do with why not} Our understanding of
ok is not bound to our own personal experiences, because
we can transcend them into an abstraction of ultimate
purpose for all men.
Page 42.
We do not drift into a new position. It
is a decision we make. In this respect it is like a
conversion experience. We cannot decide on the fourth
position without a great deal more information than most
persons have available to them about the circumstances
surrounding the original positions decided on so early
in life. Fortunate are the children who are helped early
in life to find they are ok by repeated exposure to
situations in which they can prove, to themselves, their
own worth and the worth of others. Unfortunately, the
most common position, shared by 'successful' and
'unsuccessful' persons alike, is the I'm not ok - you're
ok position. The most common way of dealing with this
position is by the playing of games.
Ber ne
defines a game as ... an ongoing series of complementary
ulterior transactions progressing to a well-defined,
predictable outcome. Descriptively it is a recurring set
of transactions, often repetitious, superficially
plausible, with a concealed motivation; or, more
colloquially, a series of moves with a snare, or
'gimmick'. {6}
I believe all games have their origin in
the simple childhood game, easily observed in any group
of three-year-olds: 'Mine Is Better Than Yours'. This
game is played to bring a little momentary relief from
the awful burden of the not ok. It is essential to keep
in mind what the I'm not ok - you're ok position means
to the three-year-old. I'm not ok means: I'm two feet
tall, I'm helpless, I'm defenceless, I'm dirty, nothing
I do is right, I'm clumsy, and I have no words with
which to try to make you understand how it feels. You're
ok means: You are six feet tall, you are powerful, you
are always right, you have all the answers, you are
smart, you have life or death control over me, and you
can hit me and hurt me, and it's still OK.
Any relief to this unjust state of
affairs is welcome to the child. A bigger dish of ice
cream, pushing to get first in line, laughing at
sister's mistakes, beating up little brother, kicking
the cat, having more toys, all give momentary relief
even though down the road is another disaster like a
spanking, getting hit by little brother, being clawed by
the cat, or finding someone who has more toys.
Grownups indulge in sophisticated
variations of the 'Mine Is Better' game. Some people
achieve temporary relief by accumulating possessions, by
living in a bigger, better house than the Joneses, or
even reveling in their modesty: I am humbler than you
are. These manoeuvres, which are based on what Adler
called 'guiding fictions', may provide a welcome relief
even thoug h
down the road may be a disaster in the form of an
oppressive mortgage or consumptive bills, which commit
the person to a life of perpetual drudgery. In Chapter 7
games are explained in detail as a misery-producing
'solution' which compounds the original misery and
confirms the not ok.
The aim of this book is to establish
that the only way people get well or become ok is to
expose the childhood predicament underlying the first
three positions and prove how current behaviour
perpetuates the positions.
Page 43.
Finally, it is essential to understand
that I'm ok-you're ok is a position and not a feeling.
The not ok recordings in the Child are not erased by a
decision in the present. The task at hand is how to
start a collection of recordings which play ok outcomes
to transactions, successes in terms of correct
probability estimating, successes in terms of integrated
actions which make sense, which are programmed by the
Adult, and not by the Parent or Child, successes based
on an ethic which can be supported rationally. A man who
has lived for many years by the decisions of an
emancipated Adult has a great collection of such past
experiences and can say with assurance, 'I know this
works'. The reason I'm ok -you're ok works is that
instant joy or tranquility is not expected.
One day a young divorcee in one of my
groups complained angrily, 'You and your damned ok bit!
I went to a party last night and I decided to be just as
nice as could be, and I decided everyone else there was
ok. And I went up to this woman I know, and I said, "Why
don't you come over and have coffee with me sometime?"
and she cut me down to two feet tall with "Well, I would
like to, but you know everybody doesn't have the time to
sit around and gas all day the way you do." It's for the
birds ... won't work!'
Personal or social storms are not going
to subside immediately when we assume a new position.
The Child wants immediate results - like instant coffee,
and immediate relief from acid indigestion. The Adult
can comprehend that patience and faith are required. We
cannot guarantee instant ok feelings by the assuming of
the I'm-ok-you're-ok position. We have to be sensitive
to the presence of the old recordings; but we can choose
to turn them off when they replay in a way that
undermines the faith we have in a new way to live,
which, in time, will bring forth new results and new
happiness in our living. The Adult also can recognize
the Child responses in others and can choose not to
respond in kind.
The change that this entails, and how
change is possible, will be illustrated in the next
chapter.
 |